Issues & Community Blog - Andrew Weaver: A Climate for Hope - Page 133

Canada needs an immediate moratorium on shipping diluted bitumen in coastal BC Waters
Media Statement January 11, 2016
Canada needs an immediate moratorium on shipping diluted bitumen in coastal B.C. waters
For immediate release
Victoria B.C. – In light of the provincial government’s final submission to the Trans Mountain National Energy Board (NEB) hearings that described BC’s spill response capacities as insufficient, Andrew Weaver, MLA for Oak Bay – Gordon Head and Leader of the B.C. Green Party, is calling on the provincial and federal governments to establish a moratorium on the transport of diluted bitumen (dilbit) along our coast.
While encouraged to see the provincial government finally agreeing our coastline is unprepared to deal with a major dilbit spill, he notes that it is inconsistent with their continued approval of the bitumen-filled tankers that travel through our marine environment – currently at the average rate of one per week.
“The BC government is admitting one thing and allowing another,” says Andrew Weaver. “In 2013 I added a 6th condition – a complete ban on the shipment of dilbit along our coast – to the province’s five approval criteria. With a dangerously low ability to deal with spills and limited scientific understanding of how dilbit will interact with BC’s waters, that 6th condition is overdue and essential.”
Trans Mountain based their entire analysis of the fate and behaviour of (dilbit) in the marine environment on the faulty assumption that dilbit floats. Published evidence, together with a Federal government study, and assessment reports from both the Royal Society of Canada’s Expert Panel on The Behaviour and Environmental Impacts of Crude Oil Released into Aqueous Environments as well as the US National Academy of Sciences Committee on the Effects of Diluted Bitumen on the Environment, all of which Andrew submitted as evidence to the NEB, clearly conclude otherwise.
In its final submission to the NEB hearings the provincial government noted that Trans Mountain had not provided adequate information on spill prevention and response, therefore not meeting a key component of the provincial five conditions required for approval of heavy oil pipelines. However the government said they will continue to evaluate the project.
“The B.C. Government submission emphasizes what I and other intervenors have been saying throughout the hearing process. There simply is not an adequate response in place now, nor likely in the future, to deal with a diluted bitumen spill.” says Andrew Weaver, “I am calling on the Federal Government to halt all current shipments of dilbit. The risk is simply too high.”
Andrew Weaver’s final argument in the Trans Mountain Pipeline Expansion Hearing Process, submitted Friday January 8th, cited “substantive deficiencies” in Trans Mountain’s application and detailed their inability to provide adequate responses to intervenor’s questions. Because of these concerns, and the NEB’s failure to include cumulative upstream and downstream effects on climate, Andrew Weaver has urged the NEB to reject their application.
-30-
Media Contact
Mat Wright
– Press Secretary, Andrew Weaver MLA
1 250 216 3382
mat.wright@leg.bc.ca

More Samples, More Questions, More Concerns: Enough is Enough
 Background
Background

On January 6, 2016 concerned Shawnigan Lake residents invited the media, politicians and the public to come and see the contaminated soil facility operating on Stebbings Road and to listen to their concerns directly. Residents, local councillors and others were in attendance to answer questions. The media and politicians were also taken on helicopter rides over the site in order to get a bird’s eye view of the operations. Indeed I was one of the many politicians who was on one such helicopter ride.
 I have written earlier on the wisdom of dumping contaminated soils in the Shawnigan Lake watershed and I have twice collected samples from the effluent running off Lot 21, immediately beside the operating contaminated soil facility.
I have written earlier on the wisdom of dumping contaminated soils in the Shawnigan Lake watershed and I have twice collected samples from the effluent running off Lot 21, immediately beside the operating contaminated soil facility.
The results of my water samples collected on April 2, 2015, together with my observation that a significant amount of fill had over run Lot 21 and was on the neighbouring parkland, led me to subsequently ask the Minister of Energy and Mines and the Minister of Environment questions during Question Period.
 The results of my sediment samples taken on May 15, 2015 at the same site as my earlier water samples led me to ask the question as to what, if anything, has been buried on Lot 21 that could produce the Thorium, Lead and other heavy metal enrichment in the sediments.
The results of my sediment samples taken on May 15, 2015 at the same site as my earlier water samples led me to ask the question as to what, if anything, has been buried on Lot 21 that could produce the Thorium, Lead and other heavy metal enrichment in the sediments.
As the months have passed, residents of the Shawnigan Lake region have continued to raise substantive concerns as to whether or not the operations at the contaminated soil facility are in compliance with the requirements of their relevant permits. On November 16th I rose in the legislature to call for an emergency debate on a recent failure of the contaminated soil site storm water containment and clarification system at the site. I did this after Island Health issued a no-water use advisory “advising residents not to use water taken out of the lake from the south end of Lake Shawnigan, south of Butler Avenue and Verlon Road, due to suspected overflow of water from South Island Aggregates’ site.” This means that residents were being advised “not to use or draw water from the area of the lake for residential or commercial use, including bathing, personal hygiene, drinking and food preparation.”
The Water Containment and Clarification System
It doesn’t end there.
 On December 1, 2015 I issued a press release calling on the BC Government to immediately cease operations at the site after the Cowichan Valley Regional District released a report from Thurber Engineering Ltd. The report identified serious concerns about surface runoff and throughflow potentially becoming contaminated but not adequately being contained or treated. In particular, the Thurber Engineering Ltd report noted that:
On December 1, 2015 I issued a press release calling on the BC Government to immediately cease operations at the site after the Cowichan Valley Regional District released a report from Thurber Engineering Ltd. The report identified serious concerns about surface runoff and throughflow potentially becoming contaminated but not adequately being contained or treated. In particular, the Thurber Engineering Ltd report noted that:
“The presence of the large volume of water emerging from under the rock armour at the head of the ephemeral stream indicates that runoff storm water sourced from the SIA site is bypassing the sediment pond (i.e by flowing under it) and is being discharged directly onto the land owned by the CVRD”.
This occurred despite the fact that the BC Government mandates that all surface water is required to be “contained on the property and treated in accordance with the permit”.
The water containment facility is shown in Figures 1a and 1c. Figures 1b and 1d illustrate a pool of water immediately beside the treatment facility. The Thurber report identifies this as potentially a source of water that feeds the ephemeral stream and bypasses the containment facility. Frankly, it would be incredibly easy to verify this by simply tagging the water with a dye as is commonly done in municipalities when potential storm/sewer crossovers are detected.
a)  b)
b) 
c)  d)
d) 
Figure 1: Photographs of the water containment system and the standing pool of water immediately beside the containment system taken on: a), b) November 16, 2015; c), d) from a helicopter on January 6, 2016.
In my view we have a serious situation where contaminated soils are being delivered to the site on an ongoing basis. Yet at the same time very troubling questions have been raised by an independent engineering firm about the functioning of the water containment system. I am beyond astounded that the Ministry would continue to allow contaminated soils to be delivered while the “permittee and their qualified professional(s)” review the situation as per the functioning of the water containment system.
I also remain troubled by the frequent referral to an ephemeral stream in numerous reports. By definition, an ephemeral stream is one that exists “only briefly during and following a period of rainfall in the immediate locality.” Yet I was given a tour of the contaminated soil facility on August 5th, 2015 and it had been very dry. At that time the stream was running and the pond was still present. This suggests to me that a component of water found in the pond has originated from below the surface.
Sulphur and Sodium Chloride Contaminants
The Shawnigan Lake residents most recently have been expressing increasing concern over the fact that contaminated soils high in sulphur and salt (sodium chloride) from Pacific Coast Terminals in Port Moody are being dumped in the operating facility.
Water in the “ephemeral creek” has been tested several times by the Ministry of Environment. The Ministry of Environment reported (see SW1) that water in the ephemeral creek (about 15m from where the containment pond discharges into it) on November 14, 2015 had:
- a sulpher concentration of 56.1 milligrams per litre
- a sodium concentration of 21.8 milligrams per litre
Samples collected by the Ministry of Environment on November 17,2015 at the same location on November 14 revealed (see E292898):
- a sulpher concentration of 23.2 milligrams per litre
- a sodium concentration of 9.16 milligrams per litre
 A summary of these results was put together in the media package provided by Shawnigan residents on January 6, 2016.
A summary of these results was put together in the media package provided by Shawnigan residents on January 6, 2016.
On the same day I took the opportunity to collect further independent samples. After the aerial tour of the site, I hiked around the property and collected two samples (Figure 2a and b) in the vicinity of where the Ministry of Environment collected their samples. I collected a third control sample in Shawnigan Creek upstream from the contaminated soil facility at almost the exact same location of where I collected my control sample in my earlier sediment analysis (see Figure 2c).
a)  b)
b) 
c) 
Figure 2: Photographs of the location of where the two water samples were taken in the ephemeral creek: a) at a location a few metres upstream from where the Ministry of Environment collected their water samples (UP POND in the January 6, 2015 water analysis data); b) at the location where the Ministry of Environment collected their water samples (DOWN POND in the January 6, 2015 water analysis data). c) Photograph of the location where I collected my control sediments for my earlier analysis. The control water sample was taken a few metres north of this location (Control at bridge in the January 6, 2015 water analysis data).
My three resulting water samples were analyzed by Jody Spence at UVic using a Thermo X-Series2 Quadrupole ICP-MS. All water samples were filtered through clean (new) polyvinyl filters (0.45 um). A separate filter used for each sample. The first 10 mL of each sample was flushed through to condition the filter before collecting the 10 mL aliquot for analysis. After filtration, the samples were acidified with 0.2 mL of 16 Molar Environmental Grade Nitric Acid.
The resulting January 6, 2015 water analysis data reveal the following results:
Sample 1: UP POND; Figure 2a
- a sulpher concentration of 33.3 milligrams per litre
- a sodium concentration of 13.5 milligrams per litre
Sample 2: DOWN POND; Figure 2b
- a sulpher concentration of 32.4 milligrams per litre
- a sodium concentration of 13.1 milligrams per litre
Sample 3: Control at bridge; Figure 2c
- a sulpher concentration that was undetectable to the limit of machine precision
- a sodium concentration of 1.85 milligrams per litre
These results are consistent with the elevated sulpher and sodium concentrations found by the Ministry of Environment back in November.
Two additional observations are worth noting. On the day I collected my samples there was no water pooled in the water containment facilities sedimentation pond (it was largely covered with snow). The pond immediately beside it was quite large and the surface appeared to be frozen. In addition, a distinct smell of sulpher hydroxide was noted at the property line where the containment facility allows water to enter the ephemeral creek.
Summary
Based on several independently-collected water samples collected over the last few months it is clear that water in the “ephemeral creek” leaving the property contains elevated levels of sodium and sulphur. The fact that sulphur was undetectable in the control sample makes it pretty clear that the contaminants originate from the Pacific Coast Terminal soils that have been dumped in the operating facility.
While it is clear to me that there is no immediate health concerns to the residents of Shawnigan Lake from the samples I collected, questions still remain. In my opinion it would be prudent for the Ministry of Environment to immediately cease operations at the facility in order to:
- Ensure the water containment facility is actually functioning as required by permit;
- Determine where the water in the pond is coming from and whether it drains into the ephemeral creek;
- Conduct an assessment as to the cumulative effects of high sodium, sulphur and potentially chemicals that will make there way to Shawnigan lake through the ephemeral creek. The site has only just opened and will be in operation for decades.
Failing to take these immediate steps I believe would be a continued dereliction of duty by the Ministry of Environment.

Media Statement – Attack on Syrian Refugees Appalling
Media Statement January 9, 2016
Attack on Syrian Refugees Appalling
For Immediate Release
Victoria B.C. – “The pepper spray attack on Syrian refugees in Vancouver is appalling” says Andrew Weaver MLA for Oak Bay – Gordon Head and Leader of the B.C. Green Party.
More than two dozen men, women and children were treated by paramedics outside the Muslim Association of Canada Centre in Vancouver the evening of January 8 as they were peppered sprayed while attending an event welcoming them to Canada.
“British Columbian’s from all communities and all walks of life have opened their hearts, homes and wallets to support refugees from Syria. It is a testament to our collective compassion and the basic values we embrace as Canadians.” says Andrew Weaver. “This attack is shocking and I want to reassure all newcomers to our communities our welcome remains as strong as ever.”
Media contact
Mat Wright
Press Secretary – Andrew Weaver MLA
mat.wright@leg.bc.ca
1 250 216 3382

Final Argument on Trans Mountain Pipeline Hearings Submitted to NEB
It has been nearly two years since I became an Intervenor in the Trans Mountain National Energy Board Hearing. My team and I spent many hundreds of hours pouring over a 15,000 page application; we submitted nearly 600 questions; we made countless motions arguing that Trans Mountain had not, in fact, answered our original questions; we’ve written numerous blog posts highlighting our concerns over the Trans Mountain pipeline proposal.
Today we submitted our 50-page final argument to the National Energy Board. As you will see from the Media Release, reproduced below, I firmly believe that the NEB should dismiss the application due to the existence of “substantive deficiencies”.
Thank you to the numerous constituents, colleagues and citizens of British Columbia who responded to our surveys, attended our town halls and emailed my office with information. I am especially grateful to the staff I had the distinct honour of working with over the lengthy intervention process: Taylor Hartrick, Evan Pivnick, Judy Fainstein, Teresa Hartrick, Claire Hume, Aldous Sperl and Mat Wright.
My final participation the hearing process will occur at 13:30 on Wednesday, January 20, at the Delta Burnaby Hotel and Conference Centre, 4331 Dominion Street, Burnaby, British Columbia. There I will be giving an my oral summary argument directly to the National Energy Board.
Media Release
Media Statement: January 8, 2016
Final Arguments on Trans Mountain Pipeline Hearings Submitted by Andrew Weaver
For Immediate Release
Victoria, B.C. – Today Andrew Weaver, MLA for Oak Bay Gordon Head and Leader of the B.C. Green Party submitted his Final Argument in the Trans Mountain Pipeline Expansion Hearing Process.
As an intervenor, Andrew Weaver argued that Trans Mountain had failed to adequately and accurately represent the full scope of risks and impacts that a diluted bitumen (dilbit) spill would have. He also stated that Trans Mountain had failed to represent a clear and satisfactory ability to respond to a dilbit spill.
“It is critical that we understand just how unprepared we are for a dilbit spill on British Columbia’s coast,” said Andrew Weaver. “This isn’t just hypothetical – we already have heavy oil tankers in our coastal waters.”
Andrew Weaver’s final argument noted that due to these “substantive deficiencies,” the application should be dismissed by the NEB.
Of particular concern in this process was Trans Mountain’s ability to respond to a spill of heavy oil. Trans Mountain based much of their analysis on the faulty assumption that dilbit would float. What little science there is available examining this issue has found that bitumen has the ability to sink in the presence of suspended particles, of which there is no shortage in British Columbia’s coastal waters.
“Trans Mountain consistently failed to provide scenarios that could sustain even the most basic scrutiny,” said Andrew Weaver. “This project needs to be halted until we better understand the science of heavy oil in marine environments and British Columbia’s spill prevention and response capabilities are greatly updated.”
A report issued by US authorities in April, 2015 warned that Canada’s major oil spill clean up protocol is decades behind their own.
Andrew Weaver applied to participate in the hearing process as both a Member of the Legislative Assembly for Oak Bay Gordon Head, and as a scientist with a doctorate in applied mathematics with a specialty in physical oceanography, atmospheric and climate science.
Andrew Weaver will be presenting his oral summary argument to the National Energy Board on Wednesday January 20th 2016 at the Delta Burnaby Hotel and Conference Centre.
-30-
Media contact
Mat Wright
Press Secretary – Andrew Weaver MLA
Cell: 250 216 3382
Mat.wright@leg.bc.ca
Twitter: @MatVic
Parliament Buildings
Room 027C
Victoria BC V8V 1X4
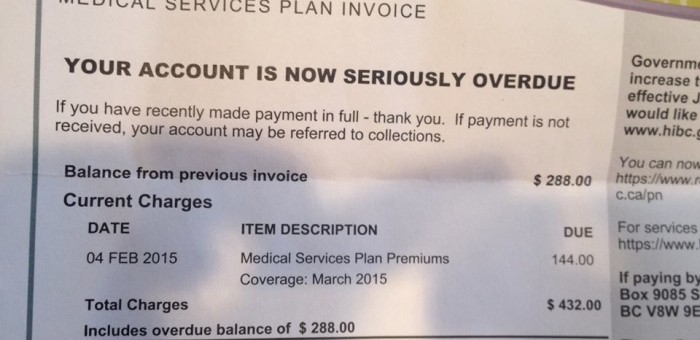
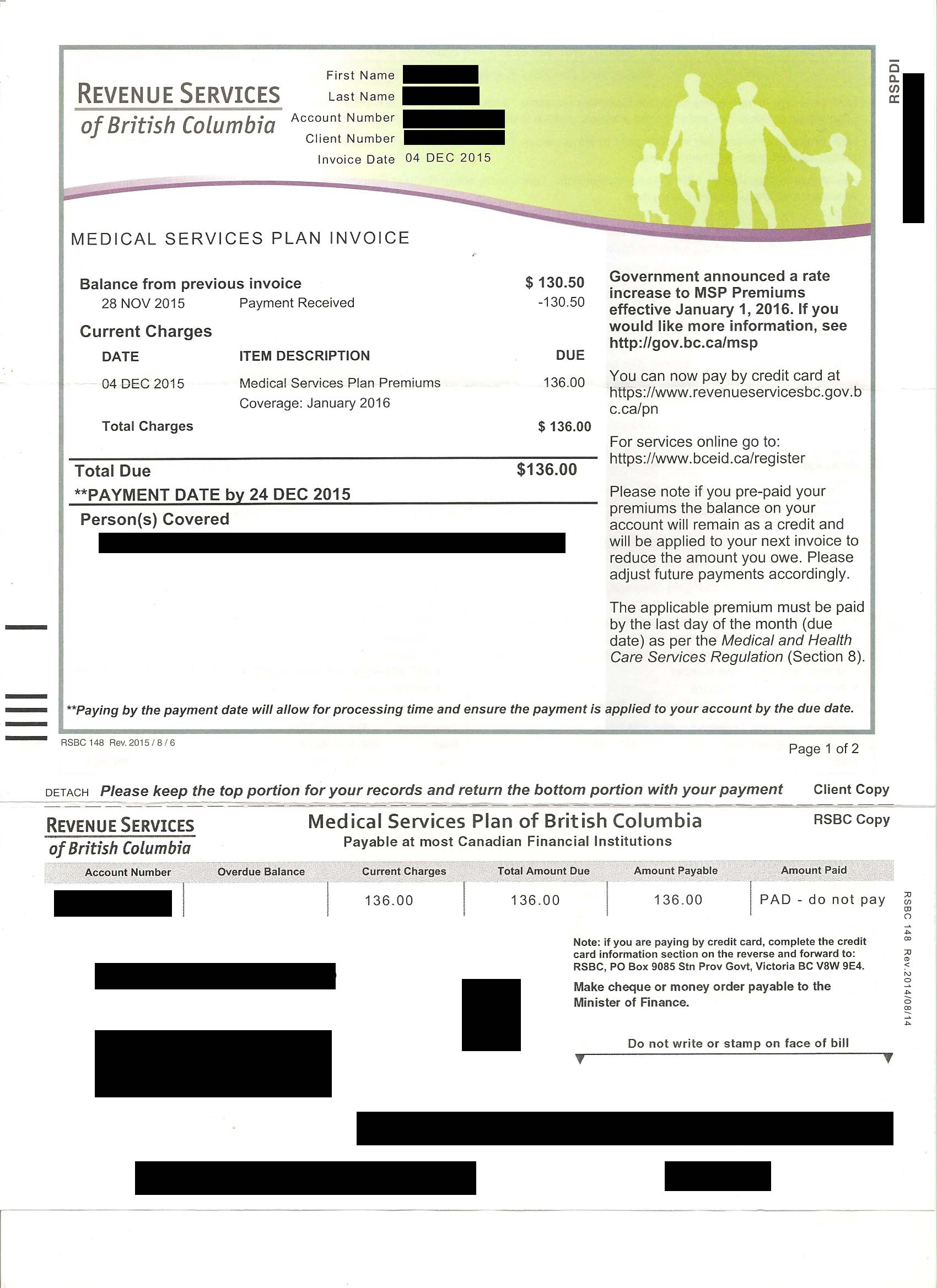
A Renewed Call to Eliminate MSP Premiums
In case you weren’t aware, life just got a little more expensive for British Columbians.
Medical Service Plan (MSP) Premiums have just gone up again. This tax is applied to anyone living in BC for six months or longer and requires them to pay monthly premiums for health care coverage. While some individuals can apply for premium assistance, these subsidies dry up as soon as a person earns a net annual income of $30,000 or more.
Healthcare costs money. There’s no denying that we need to support the medical services we rely on.
However the way MSP Premiums work in British Columbia is regressive, hurting those who can least afford it.
It’s time we followed the path Ontario has taken and rolled the MSP Premiums into our income tax system.
The Problem
 Currently in BC a person who earns $30,000 a year pays the same rate for their MSP Premiums as someone who is earning $3,000,000 a year. This is what it means to have a regressive tax – what you pay is not based on what you make.
Currently in BC a person who earns $30,000 a year pays the same rate for their MSP Premiums as someone who is earning $3,000,000 a year. This is what it means to have a regressive tax – what you pay is not based on what you make.
MSP Premiums become even more regressive when you factor in who actually pays them. The fact is, many large employers pay all or part of an employee’s MSP premium as part of a negotiated taxable benefit of employment. But for many, if not most, low and fixed income British Columbians, as well as small business owners, they must pay the costs themselves.
And they have been going up constantly.
Back in 2000, the MSP premium for a single individual was $36/month. Today that same individual pays more than twice as much, now up to $75/month. Just since 2010 there has been a 40% increase. For a family of three your new rate as of January 1st 2016 is $150/month, up from $142/month.
Let me put this another way: The BC Government rakes almost as much revenue in from MSP Premiums as it does from corporate income tax.
The government’s response has generally been to point out that it does have some premium assistance available. But this too is not without significant issues.
First, the assistance program is an opt-in program rather than an opt-out. One academic paper found that 26% of families that earned less than $30,000 a year were not enrolled in the system.
Second it would be a mistake to assume that once you are earning $30,000 a year that this is now an affordable tax.
Before moving on I’d like to acknowledge, with thanks, Lindsay Tedds at the UVic School of Public Administration for her thoughtful blog post on this issue.
MSP Premiums are a regressive tax that are contributing to the issue of affordability so pervasive in our province. What do we do about it?
The Solution
The answer to my previous question is very straightforward. British Columbia should follow the path taken by Ontario in 2004 when they introduced the Ontario Health Premium (OHP), and rolled it into their income tax system.
In Ontario if you earn $20,000 or more a year you pay the OHP. It ranges from $0 if your taxable income is $20,000 or less, and goes up to $900 per year if your taxable income is more than $200,600. Instead of the mail-out system we have in BC, the OHP is deducted from the pay and pensions of those with employment or pension income that meets the minimum threshold. The full range of premium rates in Ontario for those at different incomes can be viewed here.
Remember – only Ontario’s top earners are paying $900 per year. Right now people in British Columbia are paying $900 a year regardless of whether they earn $30,000 or $3,000,000 a year.
Next Steps
It is past time that the BC Government adopt this straightforward change. Last year, when I brought this issue up there was an outpouring of interest and support for the idea. Even the government indicated that they weren’t opposed to talking about it.
Yet, a year later, nothing has changed except that MSP Premiums have once again gone up.
This needs to be corrected. The 2016 budget will be tabled on February 16th 2016. Please join me in calling on our government to implement this common sense change for inclusion in this year’s budget.
One thing is certain, as Leader of the BC Green Party I can attest to the fact that a BC Green Party government would eliminate the regressive monthly MSP premiums. Instead, a BC Green government would introduce a progressive system in which rates are determined by one’s earnings. And a net administrative savings to taxpayers would arise in rolling MSP premiums into the existing income tax system.
Latest Posts



Recent Comments
- on The Paris Agreement is in trouble: UNFCCC needs to ratchet up their climate efforts
- on The Paris Agreement is in trouble: UNFCCC needs to ratchet up their climate efforts
- on How can BC’s environmental organizations be more effective?
- on How can BC’s environmental organizations be more effective?
- on How can BC’s environmental organizations be more effective?